

引言
现代医学理论和技术的发展,使眼科疾病的治疗水平得到了极大的提高,白内障、角膜病等大多数可致盲眼病最终得到了有效的治疗.青光眼(glaucoma),由于其对视神经造成的损害不可修复,成为 世界上第一大不可逆的致盲眼病[1-2].据联合国对2020年世界人口和世界各地流行病预测,到2020年全世界青光眼的患病人数将达到近8000万[3].我国是青光眼病高发国家. 根据青光眼的流行病学调查, 我国原发性青光眼的患病率为0.11% $\sim $1.66%.随着年龄的增长发病率也越来越高:40岁以上为1% $\sim $2%,65岁以上高达4% $\sim $7%.由此推算,我国青光眼患病人数超过800万[4-5].更为严重的是,大量青光眼患者在患病初期,由于没有症状或者症状表现不明显,很容易被忽视.据调查,在发达国家有50%的青光眼患者并不知道自己患有青光眼. 而在发展中国家该数据甚至高达90%.由于患者的视觉功能在青光眼疾病发展到晚期时已经被损害,使其无法逆转.
1 眼内压、颅内压及筛板
眼球结构如图1(a)所示. 眼内压是眼球内容物作用于眼球壁的压力(intraocular pressure,IOP).维持正常视功能的眼内压称为正常眼内压,约为10 $\sim $21,mmHg (1,mmHg=133.28,Pa). 正常情况下,房水生成率与房水排除率处于动态平衡状态,以维持正常眼内压.
图1
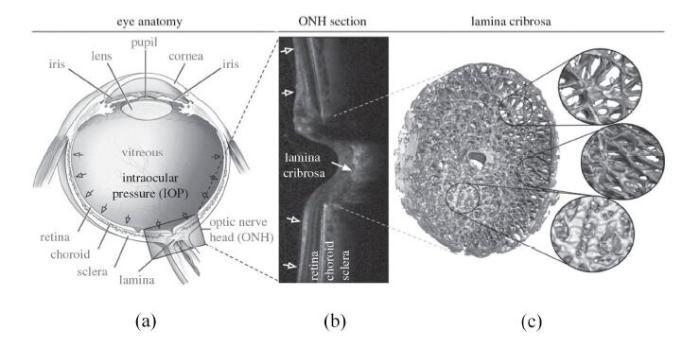
筛板位于眼球后方,是胶原纤维与筛孔中包含的视网膜神经节细胞轴突和神经胶质细胞等神经组织组成的复杂结构[14],如图1所示.其结构主要由十余层连续的纤维薄板构成,筛板周边与巩膜相连,血管和神经纤维从筛孔中穿过. 筛板半径约为0.76 $\sim $1.14,mm,平均半径为0.95,mm,厚度约为0.24 $\sim $0.36,mm,平均厚度为0.3,mm[15-17].筛板的主要作用包括:(1)支撑将视觉信号从视网膜传输到大脑的视神经节的神经突触;(2)使视网膜中心动脉和静脉穿入、穿出眼内空间;(3)调节眼内压(12 $\sim $15,mmHg)和视神经通道内组织压力(7 $\sim $10,mmHg)之间的压力差.筛板主要由睫状后动脉的分支供血,因此血液从筛板的外部边缘进入内部[18].
尽管这个关系式已被证明很好地反映了眼内压和颅内压之间的联系,但在建立青光眼发病机制的相关理论模型时,在$IOP = 20$,mmHg处关系式(1)会产生如导数不存在的一系列异常现象,这与眼内压和颅内压均由人体内连续的流体产生的生理规律不符合. 为克服这个缺陷,Tian等[23]其修正为
图2
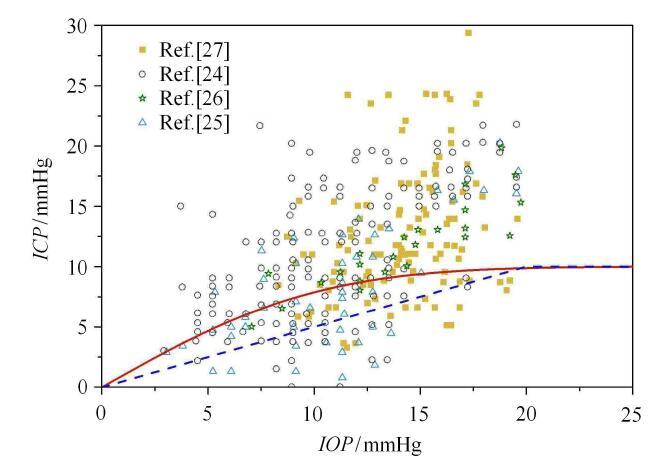
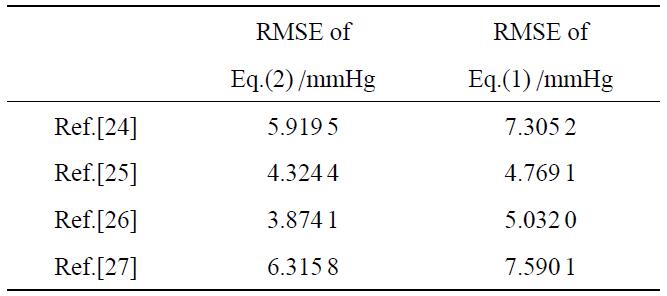
表1 基于式(1)与式(2)的理论结果相对于实验数据的均方根误差[24-27]
Table 1
 |
2 筛板变形研究
2.1 筛板组织变化
通过视神经乳头中心区域的显微照片,Yan等[28]对筛板进行了形态学检测,并测量了筛板尺度,发现眼内压升高在引起筛板变形的同时,并不会使筛板厚度发生改变.在此研究中,通过形态测定的方法使筛板的整体形状和内部结构固定.实验组和对照组分别在50,mmHg和5,mmHg载荷下对筛板加压,进行急性实验(acuteexperiment),以研究眼内压对正常视神经乳头的影响,如图3(a).在实验24,h后,虽然50,mmHg压力下筛板中心的凹陷程度(图3(c))明显大于5,mmHg压力下筛板中心的凹陷程度(图3(b)),但是二者的筛板厚度接近,即筛板在变形过程中厚度几乎不变.通过更高倍率的筛板组织显微图片发现,50,mmHg压力下筛板上结缔组织(图3(d))与5,mmHg压力下筛板结缔组织(图3(e))相比,出现了更多数目明显的横向裂纹.上述实验结果表明,眼内压在使筛板变形的过程中,并不改变其厚度;筛板边缘剪切应力在筛板变形中起主导作用,该剪切应力通过挤压视神经纤维束,使筛板上结缔组织产生横向裂纹,造成视觉区域的损失.
图3

图3
(a)固定在巩膜上的筛板(实线)示意图[28]. (b)与(c)表示在5,mmHg与50,mmHg荷载下,变形后的筛板和视神经乳头;(d)与(e)表示在5,mmHg与50,mmHg荷载下,筛板结缔组织结构图
Fig. 3
(a) Schematic view of the lamina cribrosa (solid lines) showing surrounding sclera overlain by retina[28]. Overview of the optic nerve head region from a normal human eye fixed at (b) 5,mmHg and (c) 50,mmHg; Lamina cribrosa of normal human eye fixed at (d) 5,mmHg and (e) 50,mmHg
2.2 筛孔结构变形
图4
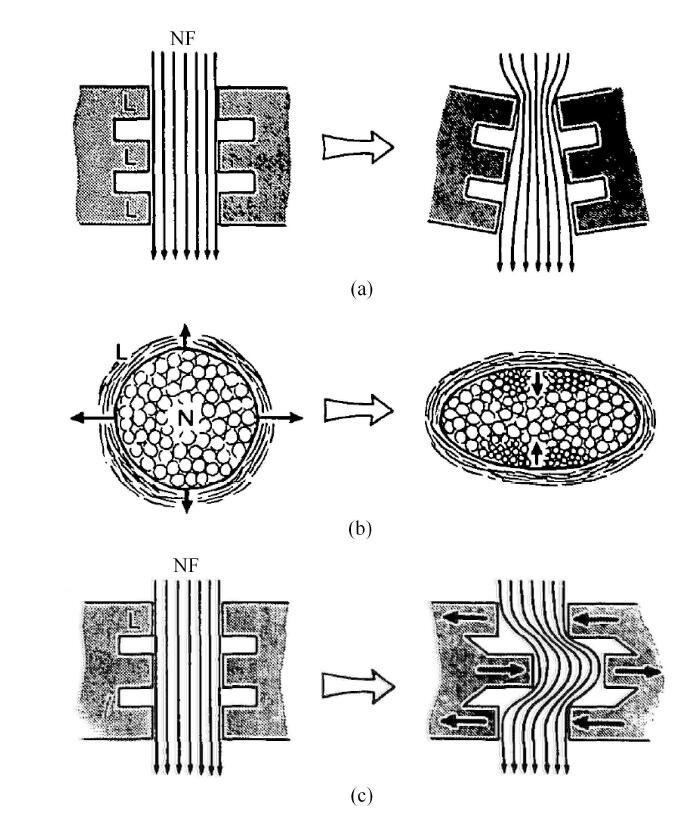
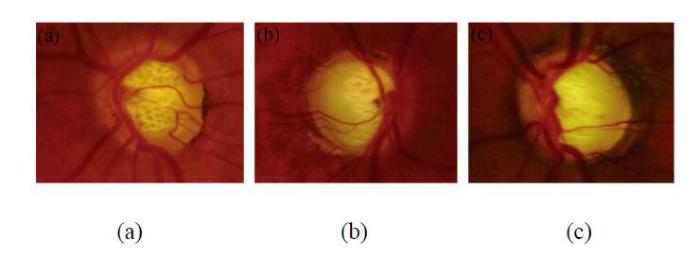
通过对青光眼患者眼底照相观察视神经盘,Tezel等[38]将筛孔形状分为3种:圆形(circular),椭圆形(oval)和有细沟的椭圆(striate),如图5所示.对高眼内压青光眼患者和正常眼内压青光眼患者的长期观察发现,这些青光眼患者可见的筛孔中,仅有7.7%是圆形的,而椭圆形筛孔和有细沟的筛孔所占比例分别为66.7%和25.6%.对比筛孔的初始形态和随后拍摄到的形态,发现青光眼病人眼内筛孔,2.6%由圆形变为椭圆形,7.7%由椭圆形变为有细沟的椭圆.在研究期间,一些患者的筛孔被拉长而变得更加细长. 同时视神经束受损加重的患者,可见的筛孔数目增多.对于单个筛孔,形状被拉长导致面积减小,而由于可见筛孔的增多,筛孔总面积增大,这些现象均伴随着神经束损伤的加剧以及青光眼病情的加重.在后续的观察发现,筛孔形状的拉长仅出现在部分患者眼中,其原因或许与治疗中减低病人眼内压从而使筛板受到的压力减小有关.
图 5
通过对青光眼病人和正常人眼内筛板进行光协调性体层摄影术(optical coherence tomography,OCT)扫描,Shoji等[47]获得了筛板的三维图像,并进行逐层比较,分析了筛孔的延伸率指标(elongation indices,EIs)与深度的关系. 研究发现,在筛板前表面上的筛孔延伸率指标最大,且在青光眼病人中更为明显.青光眼病人筛板上部(superior)和下部(inferior)受到更大的压力和弯曲,因此,这些部分的筛孔比其他部分的筛孔延伸率指标要大,且结缔组织的密度变小.这些现象表明,在筛孔延伸率大的区域,筛孔的变形使穿过其中的视神经纤维束受到了更大的不均匀的压力,筛孔的延伸率与青光眼的发病进程有关.
2.3 筛板局部变形的不均匀性
目前,研究者对眼内压升高引起筛孔变形挤压神经组织,从而导致青光眼发病这一观点已有广泛共识.Voorhees等[14]为了研究筛板的微结构和力学性能变化对视神经纤维的影响,对羊筛板的纤维定向性进行了扫描,并使用有限元的方法进行了建模和力学分析(图6).研究结果显示,在眼内压引起的筛板变形中,神经组织的应变很大且不均匀,筛板不同位置受到的应变差异也很大.筛板结缔组织的刚度和非线性影响了神经组织的应变,而神经组织的刚度和结缔组织的各向异性的影响并不明显.相比筛板中心的筛孔,筛板边缘的筛孔应变要大得多.该结果说明在筛板边缘的筛孔,其中的神经组织承受了非常大的剪切变形.通过研究眼内压对筛板上神经组织变形的影响,有助于理解青光眼的发病病理假说------视神经的损伤是眼内压引起的力学损伤.其中,值得注意的是,一些筛孔周围的组织表现出明显的应力集中现象,这一现象在靠近巩膜的筛板部分尤为明显.
图 6
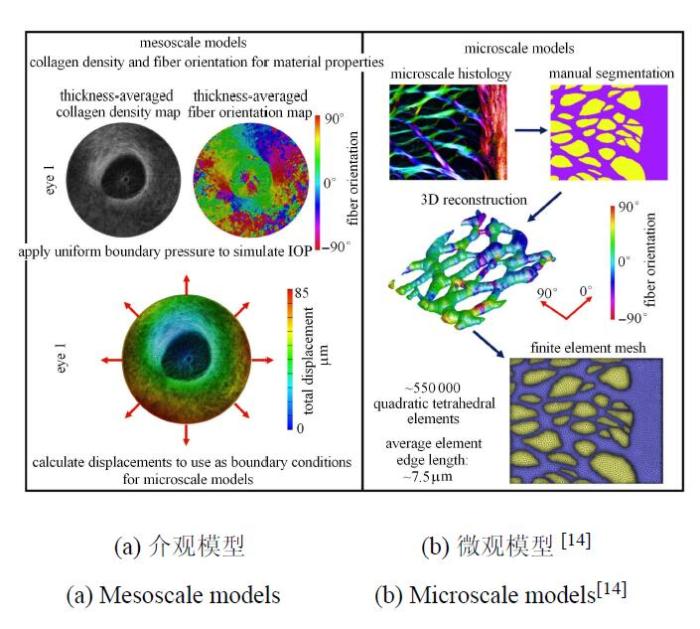
图 7
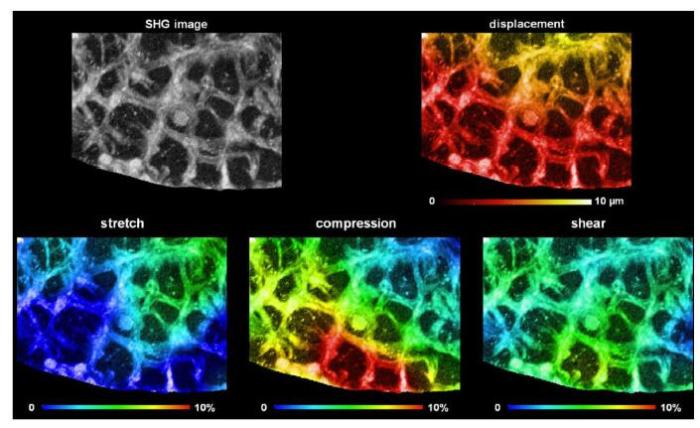
图 7
眼内压由10,mmHg增大到45,mmHg对筛板局部的影响.其中,第1行对比了筛板挠度变化. 第2行由左到右分别为筛板拉伸变形、压缩变形以及剪切变形[48]
Fig. 7
Detail of the biomechanical effects of IOP from 10,mmHg to 45,mmHg. The panels show the structure of the LC in the SHG image (top left), as well as the SHG image colored by the magnitudes of displacement (top right),stretch (bottom left), compression (bottom center), or shear (bottom right)[48]
3 筛板变形的力学模型
通过确定边界条件和测试力学参数,建立力学模型是当前理解筛板力学性能非常有效的方法.建立筛板的力学模型,目前主要考虑以下几点:(1)筛板材料的本构关系,其中主要涉及材料属性(弹性或粘性)以及相应力学参数的确定;(2)筛板与巩膜接触边界条件,其主要包括简支、固支或是附加扭转约束边界条件等;(3)筛板中是否存在预应力.
3.1 基于拉普拉斯理论的薄膜模型
图 8
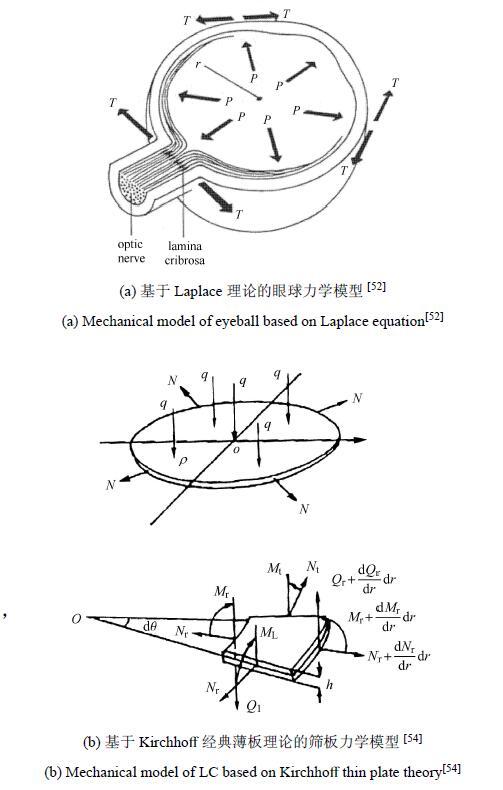
其中,$R_{S}$为眼球半径,$N$为巩膜张力.实际上,筛板在高眼内压载荷作用下,其变形包括拉伸、压缩甚至剪切[48],该薄膜模型由于忽略了筛板的厚度以及抗弯刚度且只能承受张力,因此并不适用于解决筛板问题.根据筛板的受力状态,板理论模型更适合解决筛板问题.
3.2 弹性薄板小变形模型
其中,筛板的抗弯刚度$D = Eh^{3}/[12(1-\mu^{2})]$,$E$为筛板的弹性模量,$h$为筛板厚度,$R$为筛板半径, $\mu $为泊松比, 横向载荷$q = IOP-ICP$,$I_{0}$, $I_{1}$为贝塞尔函数.在该理论模型中,文献[54]将升高的眼内压转化为横向载荷$q$和巩膜拉力$N$两个随之增大的力学载荷,提供了青光眼视神经机械损伤学说的生物力学依据.结果表明,眼内压升高会导致筛板位移增大,筛板的两个结构参数------厚度和半径,是影响筛板力学性能的主要因素:厚度影响筛板抗弯刚度,厚度越小,筛板位移越大;半径越大,筛板位移越大.
图9

3.3 弹性薄板大变形模型
其中,$k < 1$表示校正因子.研究结果表明,筛板挠度与其厚度成反比,筛板厚度增大时,筛板中心最大挠度相应减小;眼内压升高,筛板变形加剧;筛板边缘剪应力和剪应变最大.与Kirchhoff薄板小变形理论模型[54]相比,大变形理论模型[55]得到的筛板抗弯刚度要小很多.在排除了筛板几何参数对结果影响的前提下,大挠度模型所得到的挠度$w$与实验结 果[37]相差较大(图9).例如,当眼内压$IOP = 25$,mmHg和70,mmHg时,该理论模型结果与实验值之间的误差分别超过25%与30%.因此,Kirchhoff薄板大变形理论模型也不能合理体现筛板变形状态. 实际上,与筛板厚度(平均厚度300,$\mu$m)相比,筛板挠度远小于其厚度($h /w > 10$),大挠度弯曲理论假设并不成立,因此不适用于解决筛板变形问题.
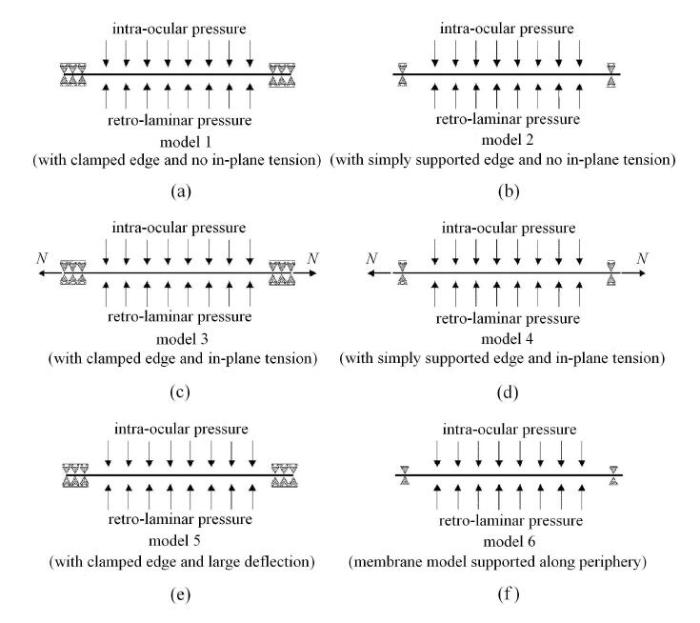
3.4 基于弹性薄板理论的六种模型
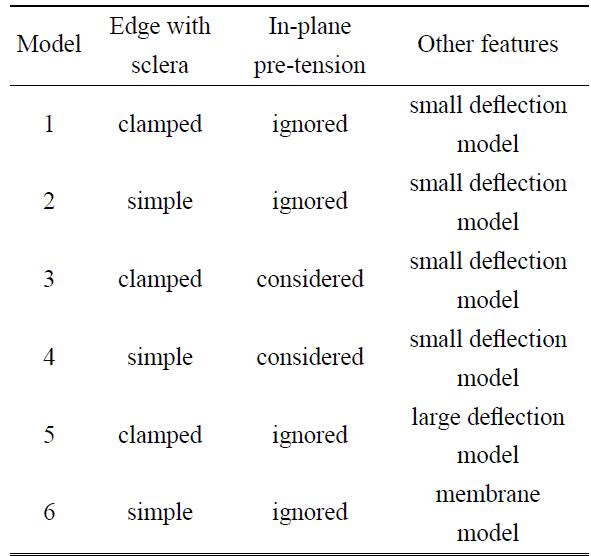
图10
3.5 基于弹性薄板理论和血流动力学的流固耦合模型
图 11

综上所述,基于拉普拉斯理论的薄膜模型仅能分析筛板承受张力的变形,忽略了筛板的厚度以及抗弯刚度,因此并不适用于解决筛板问题.筛板的层间剪切是视神经损伤的主要成因之一.然而,基于Kirchhoff经典薄板理论小变形模型、大变形模型以及流固耦合模型[18, 54-55, 58,60-61]由于其采用了直法线假设,从而使得该类力学模型不能分析筛板的横向剪切变形,限制了该力学模型的进一步应用.同时,一般薄板理论要求厚度与直径的比值小于0.1,而筛板厚度(0.24 $\sim $0.36,mm)与直径(半径约0.76 $\sim $1.14,mm)[37, 51]比值约在0.11 $\sim $0.24之间,造成采用基于Kirchhoff薄板理论的力学模型得到的结果与实验测量值误差较大.为了更深入地研究筛板变形,阐释 青光眼的发病机理,基于Reissner板理论的小变形模型近期被用于该领域的研究中.
3.6 Reissner板理论小变形模型
Tian等[46]将筛板视为小变形薄板,考虑了眼内压和颅内压对筛板的共同影响,应用Reissner板小变形理论对筛板受力变形进行力学分析.Reissner板理论对Kirchhoff薄板理论进行了修正,摒弃了直法线的基本假定,引入了板的横向剪切变形,其适用范围从薄板扩大到了中厚板.
图12
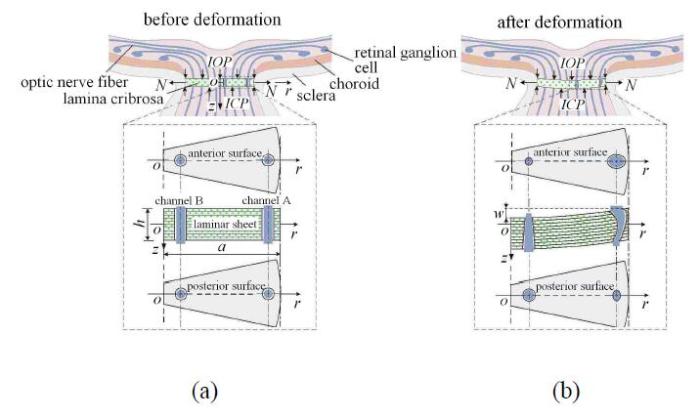
由上式可以得到,剪应变在筛板中面处最大,沿厚度方向$z$呈抛物型分布,并由筛板中心向筛板边缘处增大.
3.7 有限元方法的应用
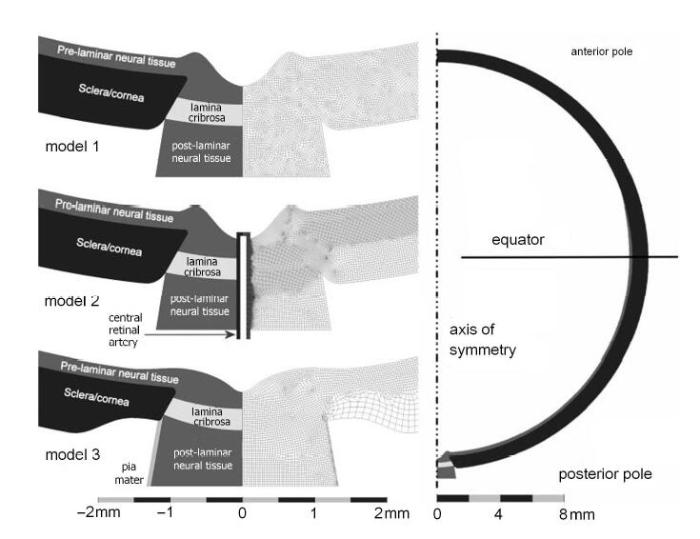
随着计算机的发展,有限元数值模拟方法已被用于计算、研究筛板的受力与变形[8-11, 48, 62-70].Bellezza等[62]采用有限元方法建立了13个理想化的眼球后巩膜壳三维几何模型,用于研究筛板变形与由眼内压造成的视乳头应力之间的关系.随后,Sigal等[48,63-67]通过建立包含筛板、筛板前后神经组织、巩膜、软脑膜及视网膜中央血管的有限元模型(图13),研究了筛板的应力、应变与变形,进而分析了视乳头的组织特性与生物力学特性,发现视乳头在与周边生物力学结构与组织协作下,可稳定地应对外界压力的变化.Yang等[69]利用有限元方法分析了在眼内压急剧增加时慢性青光眼的猴眼视神经乳头和筛板.发现筛板与巩膜可通过局部压缩变薄、伸展以及变形来弱化眼内压急剧增加对视乳头的影响.祁昕征等[68]建立了包含筛板、视网膜和脉络膜的视乳头组织三维模型.结合光相干断层扫描仪与有限元计算模型,分析了不同眼压下视网膜、脉络膜和筛板的厚度变化,通过与实验比较,证明了利用有限元法可对眼底各组织在高眼压下的形态变化进行预测的可行性.有限元方法的应用已为我们提供了大量关于筛板应力、应变与形变信息,便于我们理解青光眼的发病机理.但是由于筛板微结构的复杂性(如筛板中视神经通道(筛孔)和微板层尺寸小、结构缠结),严重地影响了有限元方法在筛板变形和损伤分析领域中的应用,如何获取更为精确的变形和受力状态,对有限元法提出了挑战.
图13
4 研究展望尽管
Tian等[46]给出了较为合理的筛板力学理论模型,但在与青光眼发生、发展密切相关的筛板变形研究中,仍有许多问题亟待解决. 首先,筛板是由胶原纤维组成的复杂网状结构,虽然可将其视为弹性圆板,但筛板上存在200 $\sim $400个筛孔,它们的存在在筛板变形中引起的应力集中问题,是青光眼发病机制研究中不容忽视的问题.在此前许多研究 中[14,49-50],提到了筛板上变形的不均匀性以及筛孔周围的高应力现象,这些现象对研究筛板变形如何引起视神经乳头损伤十分重要,而目前尚未提出明确的理论. 其次,筛板的层间横向剪切变形是视神经损伤的主要成因之一.筛板是由胶原纤维组成的复杂网状弹性结构,约可分为10层,在剪应力的作用下各层发生错动,其具体形式尚不明确.此外,目前关于筛板变形的研究主要集中在筛板自身在高眼压作用下的组织和结构变化,对于筛板变形引起的视神经乳头损伤机制研究较少,变形后的筛板如何挤压、损伤视神经乳头以及筛板变形对视神经血液循环的影响等问题仍无定论.最后,在临床上,杯盘比(视杯直径与视盘直径之比,$C /D$),是判断视神经损伤程度的重要诊断依据,正常人眼杯盘比为0.3 $\sim $0.6.青光眼患病眼杯盘比大于0.6,而在目前已有的理论研究中,无论是Kirchhoff薄板理论模型还是Reissner板理论模型,筛板杯盘比均在0.6左右且并不会随眼压升高而改变. 因此,对于青光眼患病眼的杯盘比为何会增大,仍没有合理的理论能够解释.同时,随着计算机科学的发展,借助图像识别和人工智能技术进行疾病诊断已得到应用.研究如何将光相干断层扫描(OCT)影像、眼压、杯盘比、视野与人工智能技术结合对青光眼进行诊断[71-75],不仅能够对临床青光眼的诊疗带来革命性的影响,还会带来巨大的社会经济效应.
参考文献
In vivo optic nerve head biomechanics: Performance testing of a three-dimensional tracking algorithm
Global data on blindness
The number of people with glaucoma worldwide in 2010 and 2020
北京农村及城市特定人群原发性闭角型青光眼的患病率及其影响因素
The prevalence and its effective factors of primary angle-closure glaucoma in def ined populations of rural and urban in Beijing
121697人健康体检中青光眼的筛查结果分析
Analysis of screening for glaucoma in health check-up for 121697 people
Risk factors for incident open-angle glaucoma
Relationship between intraocular pressure and primary open angle glaucoma among white and black Americans: The Baltimore Eye Survey
Reduction of intraocular pressure and glaucoma progression - Results from the early manifest glaucoma trial
Treatment of ocular hypertension and open angle glaucoma: Meta-analysis of randomised controlled trials
Optic nerve damage in human glaucoma: II. The site of injury and susceptibility to damage
Biomechanics of the optic nerve head
Reappraisal of the mechanisms of glaucomatous optic nerve damage. Eye-Transactions of the Ophthalmological Societies of the
Relationship between progressive changes in lamina cribrosa depth and deterioration of visual field loss in glaucomatous eyes
Effects of collagen microstructure and material properties on the deformation of the neural tissues of the lamina cribrosa
Cerebrospinal fluid pressure is decreased in primary open-angle glaucoma
Regional differences in the structure of the lamina cribrosa and their relation to glaucomatous optic nerve damage
Anatomic relationship between lamina cribrosa, intraocular space,and cerebrospinal fluid space
A poroelastic model for the perfusion of the lamina cribrosa in the optic nerve head
Optic nerve damage in human glaucoma: III. Quantitative correlation of nerve fiber loss and visual field defect in glaucoma, ischemic neuropathy, papilledema, and toxic neuropathy
In-vivo effects of intraocular and intracranial pressures on the lamina cribrosa microstructure
Intracranial and intraocular pressure at the lamina cribrosa: Gradient effects
Pathophysiology of optic nerve in glaucoma//McAllister JA, Wilson RP, Eds. Glaucoma. Butterworths,
A modified relation between the intraocular and intracranial pressures
Correlation of intraocular pressure with intracranial pressure in children with severe head injuries
The relationship of intraocular pressure to intracranial pressure
The relation between intracranial and intraocular pressures: Study of 50 patients
Intraocular pressure $vs$intracranial pressure in disease conditions: A prospective cohort study (Beijing iCOP study)
Deformation of the lamina cribrosa by elevated intraocular pressure
The lamina cribrosa in normal and glaucomatous human eyes
The dynamics and location of axonal transport blockade by acute intraocular pressure elevation in primate optic nerve
Radioautographic and cytochemical ultrastructural studies of axoplasmic transport in the monkey optic nerve head
Effect of intraocular pressure on rapid axoplasmic transport in monkey optic nerve
Causes of optic nerve damage in glaucoma: Robert N. Shaffer Lecture
Deformation of the lamina cribrosa and anterior scleral canal wall in early experimental glaucoma
The relation between glaucomatous damage and optic nerve head mechanical compliance
Displacement of the optic nerve head by acute changes in intraocular pressure in monkey eyes
Displacement of optic nerve head in response to short-term intraocular pressure elevation in human eyes
Alterations in the morphology of lamina cribrosa pores in glaucomatous eyes
Anatomy of the lamina cribrosa in human eyes
Quantitative regional structure of the normal human lamina cribrosa: A racial comparison
Morphometry of the human lamina cribrosa surface
The lamina cribrosa and visual field defects in open-angle glaucoma. Canadian Journal of Ophthalmology-Journal Canadien D
Comparison of optic disc features in low-tension and typical open-angle glaucoma
The clinical appearance of the lamina cribrosa as a function of the extent of glaucomatous optic nerve damage
The mechanism of optic nerve damage in experimental acute intraocular pressure elevation
Study on the deformations of the lamina cribrosa during glaucoma
Glaucomatous changes in lamina pores shape within the lamina cribrosa using wide bandwidth, femtosecond mode-locked laser OCT
Eye-specific IOP-induced displacements and deformations of human lamina cribrosa
Mapping in-vivo optic nerve head strains caused by intraocular and intracranial pressures//Larin KV, Sampson DD, Eds. Optical Elastography and Tissue Biomechanics IV,Proceedings of SPIE - The International Society for Optical Engineering,
The pressure-induced deformation response of the human lamina cribrosa: Analysis of regional variations
Factors influencing optic nerve head biomechanics
Glaucoma hypothesis: Application of the law of Laplace
Axial length and scleral thickness effect on susceptibility to glaucomatous damage: A theoretical model implementing Laplace's law
A biomathematical model for pressure-dependent lamina cribrosa behavior
Use of a mathematical model to estimate stress and strain during elevated pressure induced lamina cribrosa deformation
Mathematical modelling of the elastic properties of retina: A determination of Young's modulus
Nonlinear material properties of intact cornea and sclera
Mathematical modeling of the biomechanics of the lamina cribrosa under elevated intraocular pressures. Journal of Biomechanical Engineering-Transactions of the
Study of regional deformation of the optic nerve head using scanning laser tomography
Intraocular pressure, blood pressure, and retinal blood flow autoregulation: A mathematical model to clarify their relationship and clinical relevance
Effect of intraocular pressure on the hemodynamics of the central retinal artery: A mathematical model
The optic nerve head as a biomechanical structure: Initial finite element modeling
The Optic Nerve Head as a Robust Biomechanical System
Human Lamina Cribrosa Insertion and Age
A Few Good Responses: Which mechanical effects of IOP on the ONH to study?
A method to estimate biomechanics and mechanical properties of optic nerve head tissues from parameters measurable using optical coherence tomography
IEEE Transactions on Medical Imaging,
Finite element modeling of optic nerve head biomechanics
三维有限元模型力学分析可预测视乳头的形状变化
Shape variation of optic nerve head by mechanical analysis using three-dimensional finite element model
Deformation of the normal monkey optic nerve head connective tissue after acute IOP elevation within 3-D histomorphometric reconstructions
A methodology for individual-specific modeling of rat optic nerve head biomechanics in glaucoma. Journal of Biomechanical Engineering-Transactions of the
人工智能与青光眼:机遇与挑战
Artificial intelligence and glaucoma: Opportunities and challenges
Image processing based automatic diagnosis of glaucoma using wavelet features of segmented optic disc from fundus image
Efficacy of a deep learning system for detecting glaucomatous optic neuropathy based on color fundus photographs
Hybrid deep learning on single wide-field optical coherence tomography scans accurately classifies glaucoma suspects
Automated anterior segment OCT image analysis for angle closure glaucoma mechanisms classification

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}